0
Skip to Content
VIRTUAL APPOINTMENTS
GLP Weight Loss
Contact
Questionnaires
GLP-1 Weight Loss Questionnaire
Thyroid
Adrenal
Sleep
Gut Health
Reading
About
Reviews
Open Menu
Close Menu
VIRTUAL APPOINTMENTS
GLP Weight Loss
Contact
Questionnaires
GLP-1 Weight Loss Questionnaire
Thyroid
Adrenal
Sleep
Gut Health
Reading
About
Reviews
Open Menu
Close Menu
VIRTUAL APPOINTMENTS
GLP Weight Loss
Contact
Folder:
Questionnaires
Back
GLP-1 Weight Loss Questionnaire
Thyroid
Adrenal
Sleep
Gut Health
Reading
About
Reviews
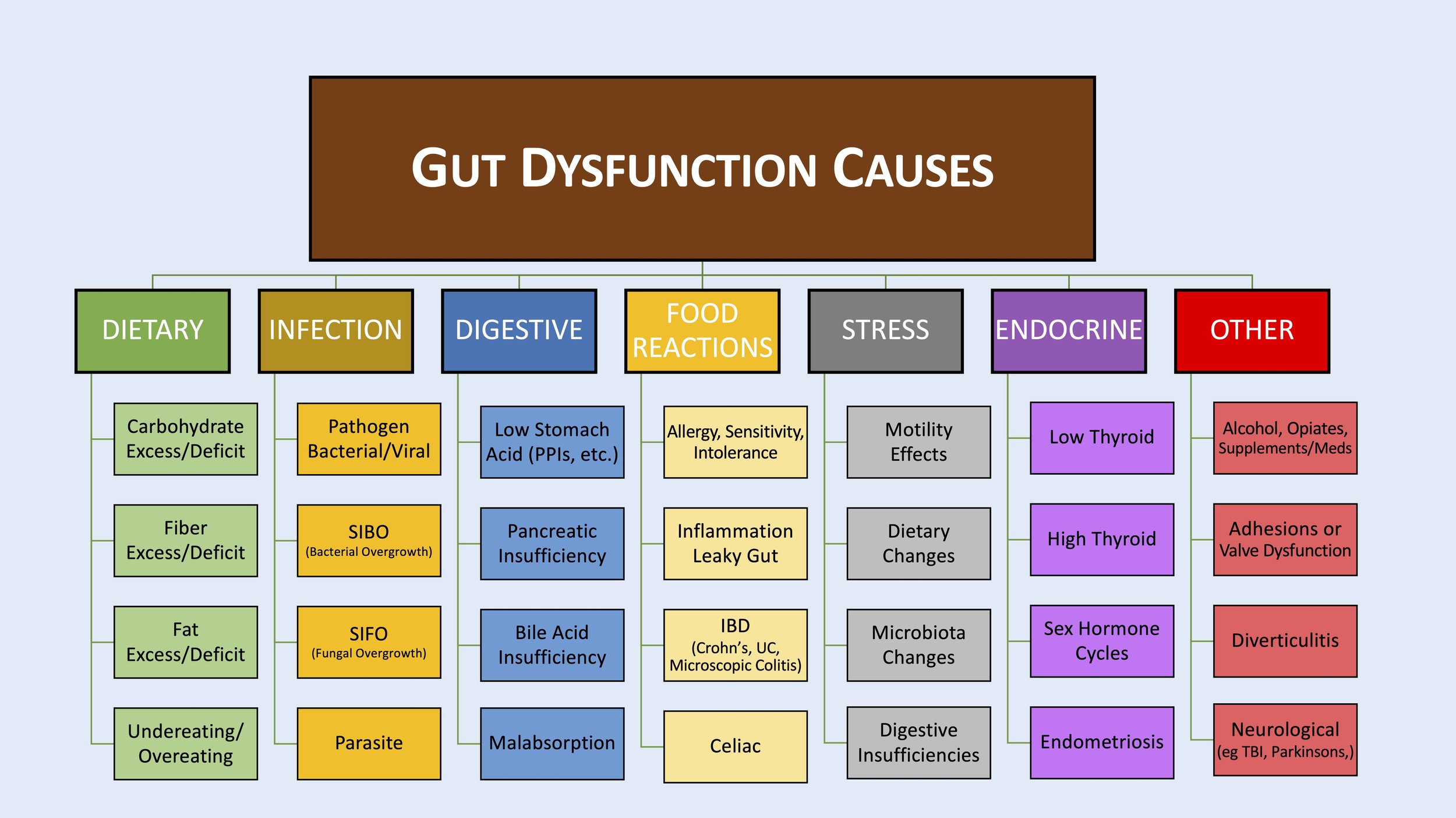
Functional Gut Health Questionnaire